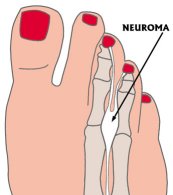
What is a neuroma?
Probably nothing is more painful than a pinched nerve. If the pinching happens in the foot, it can stop you like a frozen bearing. The condition is common and is easily caused by anything that compresses the front of the foot. The nerves in the forefoot are normally as thick as the lead in a mechanical pencil. They pass between the metatarsals on the bottom of the foot in the region of the ball of the foot with no room to spare. We have no empty spaces in our bodies; so any nerve that passes between two bones has no place to hide if the space between those bones becomes narrower.Repetitive compression can lead to thickening of the nerve. The thickening
can progress to the point where the enlarged nerve becomes as big as grape. A
nerve that has thickened to that extent is called a neuroma. Neuroma actually
means nerve tumor. A painful swollen nerve in the ball of the foot, however,
is not a true tumor. It is only an enlargement of the nerve and the nerve
sleeve. This entity has never been known to cause sickness. Its just very
painful.
The Natural History of a Neuroma
In normal walking or in good skating (as taught to me by Eddy Matzger and Barry Publow) push-off pressure starts at the heel and ends at the ball of the foot. One error in technique that may occur is over-pronation. While some pronation is normal, in over-pronation the foot rolls too much onto the inner (medial) border. In over-pronation too much inward collapse occurs. The arch excessively lowers. In this condition excess force (body weight) occurs on the inner border of the foot. Overpronation can happen in walking and running as well.Excess medial roll can lead to a threatening situation for delicate nerves that run between the long metatarsal bones. When the foot rolls excessively to the inside, the metatarsals come closer together, narrowing the space between them and pinching the nerves. Like other parts of the body, nerves can take mistreatment for a long time. Just as smokers don't get sick when they begin smoking. Continue to mistreat the body and damage will be done.
The usual progression of this type of mechanical nerve compression begins as a dull ache or a feeling of numbness in the toes or ball of the foot. The usual location involves the region of the second, third or fourth toes. Medical convention labels the big toe as the first toe. If the condition continues, pain is usually noted. Often the person senses burning pain or the feeling of a lump in ball of the foot. The sensation resembles walking on a folded up sock. If the nerve irritation (compression) continues, the pain can become severe and may even be felt at night after a hard days activity.
What Can Be Done
Start at the earliest possible time. The sooner you help the situation the better your chances are of preventing an irritated nerve from becoming a permanently thickened mass of scar tissue the unfriendly neuroma. Work on technique at the first sign of numbness, lump-like feeling or pain in ball of the foot or toes. Try to spend more push off time on the top of the wheels or outside edge of the wheels. The goal is spend less time on the inside edge pronate less. As for shoes, use shoes with a strong back section around the heel and stiff sole. The goal here is to stabilize the foot. Be sure the front part of the boot or shoe is wide enough so that it does not compress the foot. In the early stages of neuroma development consider having an orthotic made. Placing an orthotic (a professionally made shoe insert) in the shoe or boot is one of the best ways to limit over-pronation. See FaSST Autumn, page 13 for a description of what orthotics are and how they work.Anti-inflammatory medications such as Ibuprofen, Naproxen and aspirin are helpful, but only when used along with changes in the mechanical condition that is causing the problem. A podiatrist can give you a cortisone injection if the condition is severe. Dont go barefoot. Rub ice on the bottom of the foot to help reduce swelling that may exist around the nerve. MRI and CT scans are usually a waste of time; an experienced doctor will know if they are needed. Usually your description of what has happened, a plain x-ray and a good exam are enough for an experienced podiatrist to make an accurate diagnosis.
What About Surgery?
The decision as to whether to have a neuroma surgically excised is an easy one. Think of my definition of major surgery. As a board certified surgeon and teacher of surgery, I consider major surgery to be any surgery done on me. That means you should consider any surgery on you as major. Why do I say the decision is easy? Because if you cant live with the condition, it needs to be fixed. If the problem is only annoying then nonsurgical measures should be all you need. Talk it over with your foot and your doctor if surgery is being considered. Have surgery only if it is necessary. All surgery can have complications. Actually, complications from neuroma surgery are rare when an experienced surgeon does the procedure. Still the there is a small chance that numbness, infection, prolonged postoperative pain and even a regrowth of the neuroma can occur. If surgery is needed I recommend against general anesthesia. Today there is an excellent anesthesia technique involving sedation and local anesthesia. The combo produces a gentler experience and is safer than general anesthesia. The sedation makes you feel like you havent slept in days. You dont really know what is happening for about an hour. With the local anesthesia placed around the surgical site you dont feel the procedure.A neuroma can be a disabling entity. Act quickly if signs of a pinched nerve develop, doing many things yourself. Work on technique. Get the proper shoes. Use ice, medications and orthotics. See a foot doctor if these measures dont help. Consider surgery to have the neuroma removed only if all else fails.